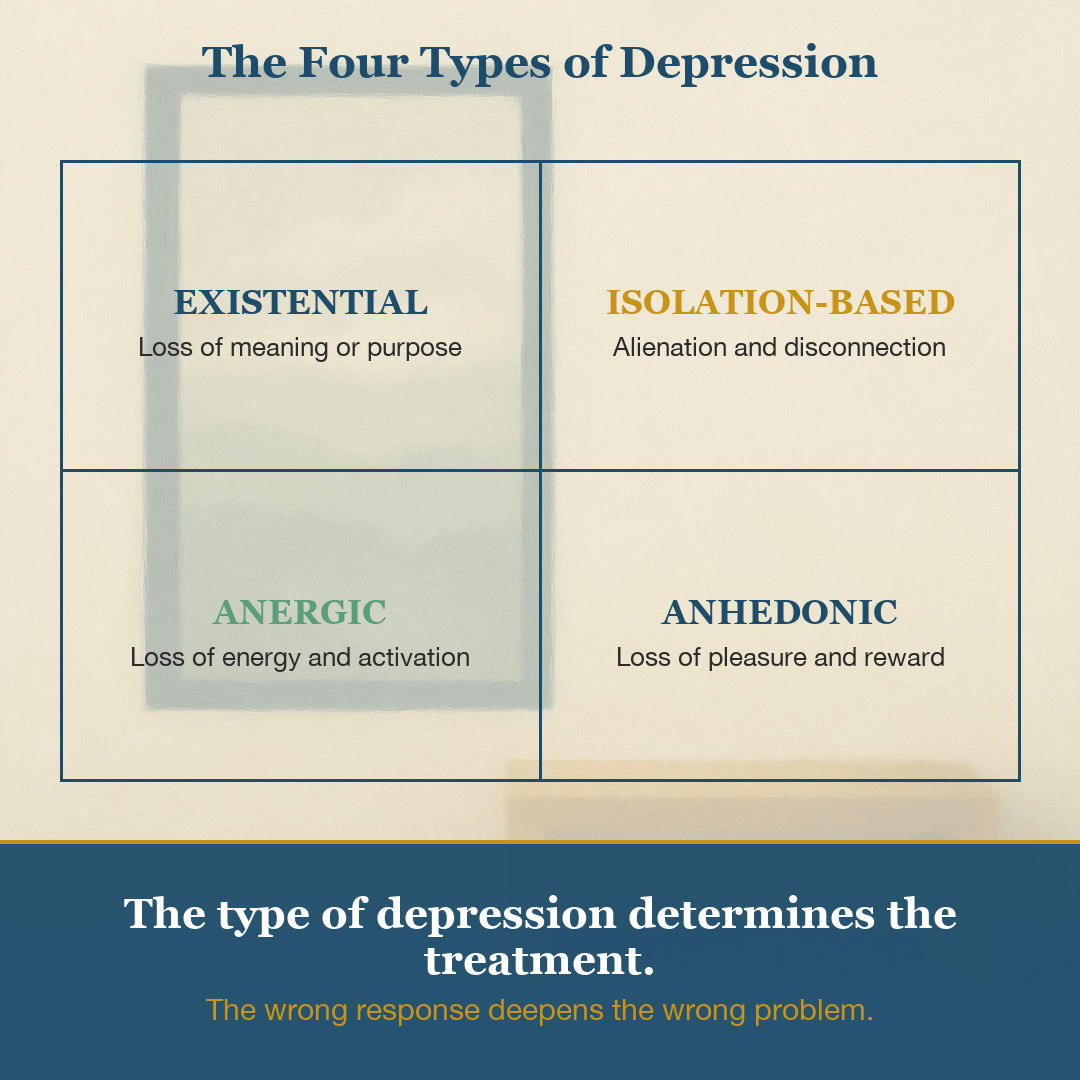
The Four Types of Depression (And Why the Wrong Response Makes It Worse)
Depression is one of the most commonly diagnosed and most commonly misunderstood experiences in modern mental health. We speak about it as though it is a single thing — a mood, a diagnosis, a chemical imbalance — when in clinical practice, what presents as “depression” is often four distinct experiences requiring four distinct responses.
Getting the category wrong doesn’t just fail to help. It can actively make things worse.
In my nine years of clinical practice, the clients who have struggled most with depression are often those who have applied the right intervention to the wrong type. They meditate when they need to move. They isolate when they need to connect. They push for meaning when the body has nothing left to give.
Here is the clinical map I use.
Type 1: Existential Depression (Meaning Deficit)
This version of depression is not primarily a mood problem. It is a meaning problem. The client is functional — they show up to work, they maintain routines, they appear fine — but inside there is a quiet flatness. A sense that nothing they are doing matters. That the effort isn’t connected to anything real.
Viktor Frankl, who survived Auschwitz and built his entire therapeutic framework around the centrality of meaning, called this kind of suffering the existential vacuum. He observed that when human beings lose contact with a sense of why, the psychological immune system collapses even in the absence of significant external hardship.
What doesn’t help: More self-reflection. Journaling inward. Asking deeper questions about the self. This type of depression is fed by hyper-introspection — the more tightly you focus on your interior, the darker the room gets.
What helps: Reorientation outward. Volunteering. Mentoring. Choosing a project that connects you to something larger than your own narrative. The goal is not to find meaning — it is to build it through contact with the world.
Type 2: Isolation-Based Depression (Alienation)
Human beings are wired for belonging at a deep neurobiological level. Social disconnection activates the same pain circuits as physical injury. This is not a metaphor. Researchers studying social exclusion found that acetaminophen reduced the emotional pain of rejection — the same drug we give for headaches.
When someone withdraws from social contact — whether from grief, shame, a move to a new city, a relationship ending, or a career transition that stripped away their professional community — the resulting depression is primarily relational. The nervous system is responding to the absence of safe connection.
What doesn’t help: Solo practices. Meditation retreats. Time alone to “figure things out.” Isolation compounds isolation.
What helps: A small, regular point of connection. Not grand social gestures — one recurring meeting, one class, one standing coffee, one community with a rhythm. The nervous system needs repetition to build trust. The goal is co-regulation, not entertainment.
Type 3: Anergic Depression (Low Activation)
This is the depression of no-energy, no-motivation, no-momentum. The client knows intellectually what they should do. The distance between intention and action feels unbridgeable. Getting out of bed feels like climbing a mountain in wet clothes.
Anergic depression often responds poorly to insight-based interventions because insight requires cognitive fuel that the system doesn’t currently have. Telling someone in this state to journal, meditate, or think more carefully about their patterns is like asking a phone with 2% battery to run a navigation app.
What doesn’t help: Complex behavioral plans. Ambitious goals. Insight work. Anything requiring sustained cognitive output.
What helps: Activation, not motivation. The clinical research on behavioral activation in CBT is clear: action precedes feeling, not the other way around. Five minutes of intentional movement, outdoors if possible. One small task completed. Momentum is not built by waiting to feel ready — it is built by starting in spite of not feeling ready.
Type 4: Anhedonic Depression (Loss of Pleasure)
Anhedonia — the clinical term for the inability to experience pleasure — is often the least-discussed and most disorienting form of depression. The client has not lost interest because they are sad. They have lost the neural capacity to feel reward. Things that used to light them up feel flat. Food, music, connection, achievement — all arrive without their usual signal.
This is not a character defect or a philosophical crisis. It is a biological shift in the reward circuitry, often following prolonged stress, burnout, or neurological depletion. The dopamine system that registers pleasure and anticipation has been chronically over-taxed or under-regulated.
What doesn’t help: More stimulation. Seeking bigger and better experiences hoping one of them will break through. This accelerates the depletion.
What helps: Savoring. High-value, low-intensity activities. Time in nature. The deliberate slow engagement with small sensory pleasures — a cup of coffee without a screen, a short walk without earbuds, cooking a meal with attention. The goal is to coax the reward system back into sensitivity, not to shock it with intensity.
The Clinical Principle Behind All Four
Each of these types is defined not just by its symptoms but by its mechanism. And each mechanism points toward a specific response. The reason depression treatment is so frequently ineffective is not because the interventions don’t work — it is because the wrong intervention is being applied to the wrong mechanism.
A person with anergic depression doesn’t need more insight. A person with existential depression doesn’t need more activation. A person with isolation-based depression doesn’t need more time alone to process.
The first clinical task is identification. Before prescribing, before advising, before recommending — the work is to understand which version of depression you are dealing with, and why.
A Note on Overlap
These four types are not mutually exclusive. In clinical practice, the majority of presentations I see are combinations — anhedonia layered on isolation, existential depression activating anergic symptoms, burnout producing simultaneous activation deficits and meaning deficits.
The framework is not a diagnostic checklist. It is a clinical lens for asking better questions: What, specifically, is missing? What specific mechanism is driving this? And what specific response does that mechanism actually call for?
Getting those questions right is the beginning of genuinely useful work.
Jagdeep Chadha is a Licensed Professional Counselor and founder of Being Counseling, PLLC in Houston, TX. He holds a Master’s degree and professional doctorate in Psychological Counseling from Columbia University, Teachers College, and spent seventeen years in senior leadership in higher education before entering full-time clinical practice. He works with high-performing individuals seeking concierge-level psychotherapy. Learn more at beingcounseling.com.